DHT and hair loss: how the hormone shrinks your follicles — and what LLLT laser therapy actually does about it
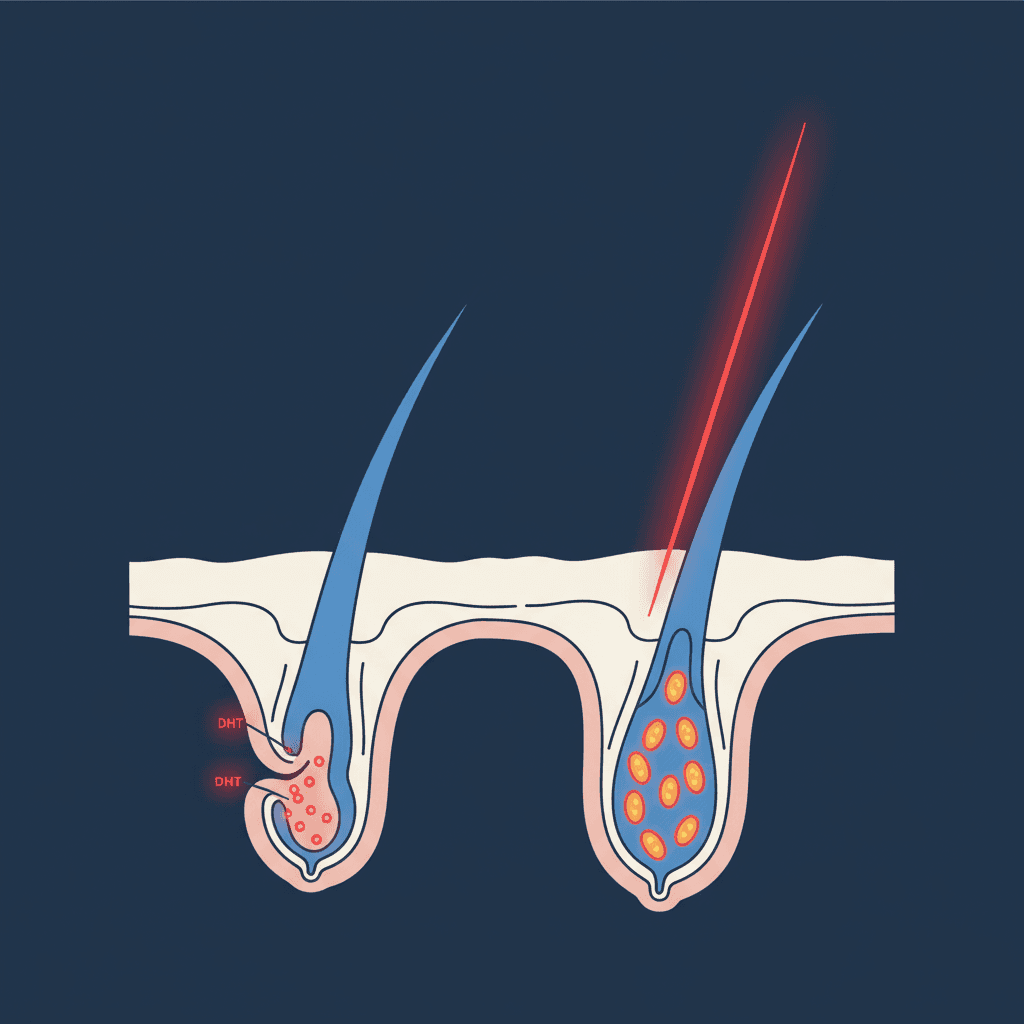
Table of contents
Short version — DHT (dihydrotestosterone) is, in genetically susceptible people, the driver of pattern hair loss: it binds to androgen receptors in the hair follicle and pushes it through smaller and smaller cycles until only vellus hair — or nothing — is left. LLLT laser therapy does not meaningfully lower your DHT; only finasteride or dutasteride does that. What LLLT does do is protect the follicle from the damage DHT causes: more ATP in follicle cells, less oxidative stress, a longer growth phase. That's why LLLT works well alongside a DHT blocker, not as a replacement.
If you start reading seriously about hair loss, you arrive at one molecule very quickly: DHT. Forums, dermatologists, the finasteride leaflet — it's everywhere. But what DHT exactly does to your follicles, and where laser therapy (LLLT) fits into that story, often stays vague. "Does a laser cap lower my DHT?" is one of the most common questions we get, and the honest answer is: no, not in any meaningful way — and that's also not how laser therapy works. Time to lay that out properly.
Full disclosure: I work at Lascure, we sell laser caps. So I have an obvious interest in you understanding what laser therapy can do. That's exactly why I want to be honest about what it cannot do — because claims that LLLT "blocks DHT" simply aren't what the science says, a few cautious in-vitro signals aside.
What is DHT exactly, and where does it come from?
DHT stands for dihydrotestosterone. It's an androgen — a male sex hormone — produced by both men and women, just in much higher amounts in men. Your body doesn't make it directly; it converts testosterone into DHT via an enzyme called 5-alpha-reductase. That enzyme sits in your hair follicles, prostate, sebaceous glands and skin, among other places.
DHT itself is useful. It's responsible for much of male development at puberty: beard growth, body hair, deeper voice, reproductive system development. The problem isn't DHT itself — the problem is how some hair follicles respond to it.
There are two variants of 5-alpha-reductase. Type II lives mainly in the scalp (and prostate) and is what finasteride inhibits. Type I sits more in the skin and sebaceous glands; dutasteride inhibits both. How active this enzyme is in your scalp — and how sensitive your androgen receptors are — is largely genetic. That's the "hereditary" in hereditary hair loss.
How does DHT actually cause hair loss?
A hair follicle isn't a passive hole in your skin; it's a small, physiologically active mini-organ. At its base sits a structure called the dermal papilla — a cluster of cells that act as a kind of control room. The dermal papilla decides how long the hair grows, how thick it gets, and when the follicle starts a new cycle.
Here's the crux: in genetically susceptible people, androgen receptors sit in and around that dermal papilla. DHT binds to those receptors like a key in a lock. Once the lock turns, the papilla changes its program — not abruptly, but gradually over many hair cycles. Concretely, roughly this happens:
- The anagen (growth) phase shortens. A healthy hair grows for 2–6 years. Under DHT pressure, that phase gets shorter each cycle, sometimes down to a few months.
- The follicle shrinks. Each new cycle starts with a slightly smaller follicle. This is miniaturisation: a terminal hair (thick, pigmented, long) gradually turns into a vellus hair (short, thin, colourless fluff).
- The resting (telogen) phase lengthens. The gap between a hair shedding and a new one growing gets longer — so your scalp looks balder, even though the follicle isn't entirely dead.
- Local inflammation and oxidative stress. DHT-bound follicles produce more inflammatory signals (such as TGF-β and interleukins) and show elevated oxidative stress in their cells' mitochondria — which weakens things further.
This is why male pattern baldness has a typical pattern (receding hairline, crown thinning) and female pattern baldness another (diffuse thinning over the crown with the hairline preserved): those zones have the highest density of androgen receptors and the most 5-alpha-reductase activity. The sides and back of your head, by contrast, are relatively DHT-resistant — which is why those regions are used as donor sites in hair transplants.
What actually lowers DHT?
Before we talk about lasers: there are only a few interventions that we can confidently say lower DHT. Both are medications:
- Finasteride inhibits 5-alpha-reductase type II and lowers scalp DHT by roughly 60–70%. Clinical trials consistently show it slows hair loss and produces moderate regrowth in a majority of users.
- Dutasteride inhibits both type I and type II and lowers DHT even more (around 90%); used off-label for hair loss in countries like South Korea and Japan.
Topical minoxidil does not lower DHT — it works through a different mechanism (vasodilation, anagen extension via potassium channels). Supplements like saw palmetto, pumpkin seed oil and green tea extract are often marketed as "natural DHT blockers", but the evidence is thin and mostly limited to small or in-vitro studies. To be honest: none of them come close to finasteride for DHT reduction.
So what does LLLT laser therapy do about DHT?
Here's the honest nuance you rarely see in marketing copy: LLLT does not meaningfully lower your DHT levels. A few in-vitro studies and small papers suggest photobiomodulation might have a local effect on 5-alpha-reductase activity, but this is not a robust effect and it's not how the major clinical trials explain their outcomes.
What LLLT actually does is something different — and arguably just as interesting. Red laser light in the 630–670 nm range is absorbed by cytochrome c oxidase, an enzyme in your cells' mitochondria, including the follicle cells stressed by DHT. That process — photobiomodulation — has a number of measurable effects:
- More ATP. Mitochondria produce more cellular energy. Follicle cells pushed into a low-energy state by DHT get fuel to do their normal work again.
- Less oxidative stress. Reactive oxygen species (ROS) — elevated in DHT-bound follicles — are dampened; the cell's antioxidant systems activate.
- Longer anagen phase. Animal models and clinical trials show LLLT keeps follicles in a more active, longer growth phase — the opposite of what DHT does.
- Less local inflammation. Markers of micro-inflammation in the follicle environment decrease.
In other words: LLLT doesn't tackle DHT at the source — it protects the follicle from the damage DHT causes. Finasteride closes the tap; LLLT reduces the water damage.
The clinical evidence for that protective effect is solid. Jimenez et al. (2014) ran a randomised, double-blind, sham-controlled trial with 269 men and women and found a significantly larger increase in hair density in the laser cap group. Kim et al. (2013) confirmed this in a separate multicentre trial. Afifi et al. (2017) pooled several RCTs in a meta-analysis in Lasers in Surgery and Medicine and concluded that LLLT significantly increases hair density versus placebo.
Why LLLT and finasteride complement each other
Once you line up the mechanisms, it becomes clear why dermatologists often recommend a combination:
- Finasteride reduces the signal that's slowly miniaturising your follicles.
- LLLT improves the health and energy state of follicles that haven't fully miniaturised yet.
- Minoxidil extends the anagen phase and improves perfusion.
Three different angles on the same problem. Combination-therapy studies (LLLT plus finasteride, or LLLT plus minoxidil) suggest the effects add up — which is consistent with what you'd predict from the mechanisms.
For people who can't or don't want to take finasteride — because of side effects, family planning, or simply preference — LLLT is often used as a cornerstone together with minoxidil. The treatment effect is smaller without finasteride in the mix, but still measurable.
Does every "red light cap" work against DHT damage? No.
This is where a lot of people waste money. "Red light" isn't a synonym for "medical laser". To get the effect on follicle cells that the studies above demonstrated, you need three things:
- Real laser diodes, not just LEDs. Laser light is coherent and monochromatic; LED light isn't, and penetrates less deeply to where the dermal papilla sits. The published trials almost all used laser diodes.
- The right wavelength: 650–670 nm. This is the range where cytochrome c oxidase absorbs best. Caps running at 630 or 700+ nm miss the window.
- The right dose. Clinical devices deliver around 4–5 mW per diode, with sessions of 25–30 minutes a few times per week. A €40 cap with 50 weak LEDs doesn't reach that dose.
We covered that in a separate post: is red light therapy for hair a scam? Spoiler: it isn't — but many of the caps sold under that label, unfortunately, are.
What can you realistically expect?
Honest, here too:
- LLLT is no miracle. The effect is modest — more hair than without treatment, thicker hair than without treatment, but not a full head of hair on a bald crown.
- Earlier is better. LLLT (and finasteride, for that matter) works best on follicles that haven't fully miniaturised yet. In a zone that hasn't grown anything for years, there's little left to protect.
- It's a long-term treatment. Expect first differences after 16–24 weeks of consistent use, and think of it as maintenance, not a course of treatment.
- Your DHT stays the same. Stop LLLT, the protection ends — and DHT picks up where it left off. The same is true, by the way, for finasteride and minoxidil.
Conclusion
In pattern hair loss, DHT is the cause: it binds to androgen receptors in the follicle and triggers miniaturisation. If you want to lower DHT itself, finasteride (or dutasteride) is the only intervention with serious evidence behind it. LLLT laser therapy doesn't lower DHT, but makes your follicles more resilient to what DHT is trying to do to them — more mitochondrial energy, less oxidative stress, a longer growth phase. For people who'd rather avoid systemic DHT inhibitors, or who want to stack treatments, LLLT is a serious, clinically supported option — provided the device uses real 650 nm laser diodes and delivers the right dose.
One note: this article is informational and isn't medical advice. For a treatment plan tailored to your situation — especially if you're considering medication — talk it through with a dermatologist or your GP.
More articles
Do laser helmets really work against hair loss? What science says
Discover what clinical research says about laser helmets for hair loss. An honest, science-backed analysis without overclaims.
Stop Hair Loss: 6 Proven Methods Honestly Compared
Your hair is thinning and you want to do something about it. But what actually works? We compare six treatments — from hair transplants to DHT blockers — on effectiveness, cost, and what you can realistically expect.

LLLT vs hair transplant: which is better for you?
A hair transplant delivers the most visible results, but costs thousands and requires surgery. A laser helmet works more gradually, but without cutting, without side effects, and at a fraction of the price. Which is the right choice?